When Did You Stop Feeling Like Yourself?
You used to have energy to spare. The drive, the focus, the strength — it was just there. Now it takes twice the effort to get half the result, and nobody seems to have a real answer.
9-minute audio overview — how testosterone works, delivery methods, and your expected timeline
Full Testosterone deep-dive
What Is Testosterone?
You wake up exhausted even after eight hours of sleep. Your workouts feel half-hearted. Your mind clouds over by 3 p.m. The drive that once defined you — sexual, professional, athletic — has quietly dimmed. You’ve tried better sleep, stricter training, supplements. Nothing sticks. The problem isn’t discipline or willpower. It’s biochemistry.
Testosterone is your body’s primary male sex hormone and the most potent endogenous androgen 3. It fuels energy production, muscle growth, fat loss, sexual desire, mood stability, and cognitive sharpness. When it declines — whether through aging, metabolic disease, or life stress — everything slides. The fatigue becomes real. The decline becomes measurable.
The good news: hypogonadism, the clinical term for low testosterone, is treatable. And it’s common. At 60, roughly 19% of men fall below the optimal range. By 70, that number climbs to 28%. By 80, it reaches 49% 7. You’re not alone. The normal testosterone range is 300–1,000 ng/dL 7. If your lab results place you below that, or if symptoms align with deficiency, testosterone replacement therapy (TRT) can restore what aging or metabolic stress has taken.
Zvia Weight Loss & MedSpa approaches testosterone replacement with the same precision and care we bring to every other therapeutic protocol: comprehensive lab testing, individualized dosing, ongoing monitoring, and integration with your lifestyle. This deep dive explains how testosterone works, what you can expect, and why the right protocol — delivered and managed by people who know you — makes all the difference.
How Does It Work?
Testosterone’s effects ripple through your body via two primary mechanisms: genomic (slow, sustained) and non-genomic (fast, cellular).
Genomic pathway: Testosterone crosses the cell membrane and binds to the androgen receptor (AR/NR3C4) in the cytoplasm 3. The hormone-receptor complex travels into the nucleus, where it attaches to androgen-responsive elements (AREs) on DNA 3. This triggers gene transcription, activating the production of proteins responsible for muscle growth, fat metabolism, bone density, and metabolic health.
Tissue-specific conversion: Once inside cells, testosterone is converted into two specialized forms. The enzyme 5α-reductase transforms testosterone into dihydrotestosterone (DHT), a more potent androgen that drives hair, skin, and prostate tissue effects 3. Meanwhile, the enzyme aromatase converts testosterone into estradiol, the primary female sex hormone, which is critical for bone health, cardiovascular protection, and cognitive function in men 3. This dual pathway ensures testosterone’s benefits are distributed across multiple systems.
Non-genomic signaling: Beyond the nucleus, testosterone activates rapid signaling cascades — Src, Raf-1, and Erk-2 kinases 3 — that produce immediate cellular effects. These fast pathways enhance muscle contraction, improve blood vessel function, and support mood and sexual arousal within hours or days, not weeks.
The result: testosterone doesn’t just make you stronger or more sexual. It rewires your metabolism, mood, cognition, and resilience at the cellular level.
What Are the Benefits of Testosterone Therapy for Men?
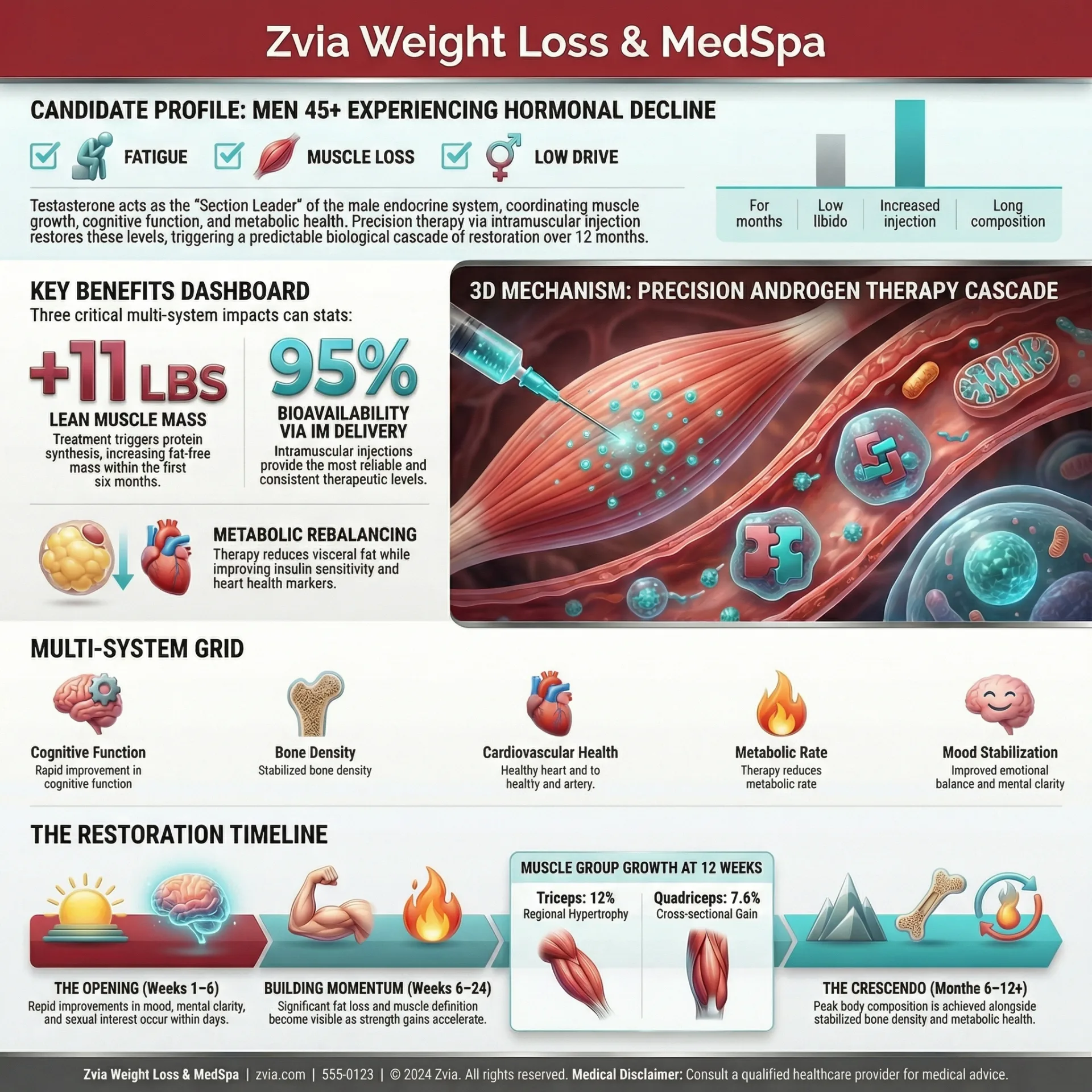
Lean muscle mass restoration. Testosterone activates AR-mediated protein synthesis in skeletal muscle, shifting your body toward growth and away from catabolism. Men on TRT typically gain 3–5 kg of lean mass over three to six months, even without aggressive training — and with resistance work, gains accelerate.
Body fat reduction. Testosterone activates AR signaling in adipose tissue, triggering lipolysis and increasing metabolic rate 1. Fat preferentially mobilizes from the abdomen and viscera, the deposits most linked to cardiovascular and metabolic disease. Combined with proper nutrition and activity, TRT reduces body fat within six months 1.
Energy and vitality. Testosterone drives mitochondrial biogenesis — the creation of new energy-producing machinery inside your cells 1. It also stimulates erythropoiesis, the production of red blood cells, which carry more oxygen to tissues 1. You don’t just gain energy; you gain sustained endurance and the mental clarity that comes with better oxygen delivery to the brain.
Sexual function recovery. TRT enhances erectile function, increases sexual desire, and restores sexual satisfaction 5. These improvements are rooted in AR expression in the corpus cavernosum (penile tissue) and the central nervous system. You recover not just physical capacity but psychological confidence.
Mood stabilization and cognitive clarity. Testosterone acts on AR-expressing neurons in the limbic system — the brain’s emotional and memory center 1. Men report reduced irritability, improved focus, and a return of motivation and optimism. The effect is subtle but profound: you feel like yourself again.
Bone mineral density protection. Testosterone stimulates osteoblasts (bone-building cells) directly via AR signaling 3. The aromatase conversion to estradiol adds a second protective pathway for bone health, critical for preventing osteoporosis and fractures as you age.
How Long Does Testosterone Therapy Take to Work?
Testosterone replacement unfolds in three distinct phases, each with its own milestones. Individual variation is real — genetics, baseline hormone levels, lifestyle factors, and stress all influence the exact pace. But the sequence is reliable.
Phase 1 — The Opening (Weeks 1–6): The first signals arrive early. Energy and mood shift within the first one to two weeks as non-genomic pathways activate 1. In our practice, the first thing most men notice isn’t the gym performance — it’s the mood. Clients regularly describe feeling like a fog has lifted within the first three to four weeks of optimization. Sexual interest returns around week three and plateaus by week six 1. Overall quality of life improvement registers at weeks three to four 1. These early wins are psychological anchors; they confirm the protocol is working and keep you engaged.
Phase 2 — Building Momentum (Weeks 6–24): This is where the deeper transformation happens. Visible body composition changes emerge at weeks eight to twelve; by month three, most men see measurable muscle gain and fat loss 1. Strength gains accelerate six to twelve weeks in 1. Mood reaches maximum improvement by week eighteen to thirty, a window longer than most expect but worth the patience 1. Red blood cell production (erythropoiesis) begins in week three but peaks at three months 1. Lipid profiles (cholesterol, triglycerides) begin shifting within four weeks and stabilize around twelve weeks 1. You’re not just feeling better; your bloodwork is improving.
Phase 3 — The Crescendo (Months 6–12+): Stabilization and sustained optimization. Bone mineral density improvements continue through nine to twelve months 1. Lean muscle mass plateaus at an equilibrium reflecting your training stimulus and nutrition. Energy and sexual function remain stable. For many men, this is the phase where TRT becomes seamless — no longer novel, but thoroughly integrated into your life.
Timeline Note: Individual variation reflects genetics, age, baseline hormone levels, training consistency, nutrition adherence, sleep quality, and stress management. Some men see body composition changes in month two; others need month three or four. Sleep deprivation (five hours nightly vs. normal sleep) reduces testosterone by 10–15% 9, underscoring why lifestyle integration matters. A provider who monitors your labs and adjusts your protocol based on your unique response curve achieves better outcomes than one following a generic template.
Is Testosterone Right for You?
The ideal candidate presents with both measurable hypogonadism (lab confirmation, usually below 300 ng/dL) and clinical symptoms: fatigue, strength loss, sexual dysfunction, mood decline, or cognitive fog. We often think of two archetypes.
The Relief Seeker has experienced a clear decline — aging, metabolic disease, or chronic stress — and wants restoration to a baseline that felt normal. This is often a man in his 50s, 60s, or 70s recovering the function and vitality of a decade prior.
The Optimization Pursuer may have low-normal or borderline-low testosterone and wants to maximize performance, body composition, and resilience. This is often a younger man (40s–50s) seeking competitive edge or a midlife refresh.
Both profiles respond well to TRT when baseline labs confirm the need and when the protocol is tailored to the individual.
Provider evaluation is the definitive step. A comprehensive lab panel — total testosterone, free testosterone, estradiol, DHT, SHBG, lipids, liver function, hemoglobin, PSA, and metabolic markers — determines eligibility, guides dosing, and establishes monitoring baselines. Contraindications include untreated sleep apnea, severe untreated hypertension, prostate cancer, breast cancer, or severe polycythemia 7. A provider with deep knowledge of your medical history makes this evaluation trustworthy.
Safety data is reassuring. The TRAVERSE trial, which enrolled 5,246 men and tracked major adverse cardiovascular events, found no increased cardiovascular risk in men receiving TRT (7.0% vs. 7.3% event rates) 2. The FDA removed cardiovascular black box warnings in 2025 8. The TestES meta-analysis of 35 trials involving 5,601 participants confirmed TRT safety across populations 6. And contrary to fear-based narratives, TRT does not exacerbate benign prostate hyperplasia or increase prostate cancer risk 5.
These data support TRT as a safe, evidence-based intervention when properly monitored.
What Does a Testosterone Protocol Involve?
Testosterone replacement via Zvia utilizes two delivery methods, each with distinct pharmacokinetics and advantages.
Intramuscular (IM) injection: Delivered weekly or biweekly, IM testosterone (enanthate or cypionate formulation) achieves ~95% bioavailability 10. Enanthate has a half-life of approximately 4.5 days; cypionate approximately 8 days 10. IM delivery produces stable, physiological testosterone levels when dosed appropriately. Weekly dosing typically ranges from 50–100 mg; biweekly doses scale accordingly. The protocol is straightforward: a brief injection, minimal training disruption, and reliable absorption. Most men report ease and confidence with IM within the first month.
Subcutaneous pellet implant: Testosterone pellets — bioidentical crystalline form, 75 mg per pellet — are placed subdermally (under the skin) in a small incision, typically in the lower abdomen or hip 4. A typical protocol uses 6–12 pellets (450–900 mg total), with duration of three to six months 4. Pellets provide ~100% bioavailability 4 and release testosterone steadily via a 2.5-month absorption half-life 4, producing a steady-state release of approximately 1.3 mg/day per 200 mg of pellet mass 4. Patient satisfaction with pellets exceeds 70% 4. The advantage: no weekly injections, no monthly pharmacy visits, no compliance burden. The trade-off: an in-office procedure, a brief healing period, and a six-week lead time before full absorption. For men seeking set-and-forget simplicity, pellets often win.
Delivery comparison:
| Feature | IM Injection | Pellet Implant |
|---|---|---|
| Bioavailability | ~95% | ~100% |
| Frequency | Weekly or biweekly | Every 3–6 months |
| Onset | Days to 1 week | 2–4 weeks |
| Steady-state | Immediate | 2.5–3 months |
| Procedure | Injection | Minor surgical incision |
| Patient burden | Ongoing visits | Single procedure, then months off |
Your provider determines the optimal method based on your preference, lifestyle, compliance history, and medical profile. Neither is universally better; each suits different patients.
Lifestyle integration is non-negotiable. Testosterone therapy amplifies the benefits of good fundamentals and reveals the limits of poor ones.
Nutrition: Adequate protein (1.6–2.2 grams per kilogram of body weight daily) and micronutrient sufficiency — zinc, magnesium, vitamin D3 — support the anabolic response. Iron status should be monitored, as TRT stimulates red blood cell production.
Activity: Resistance training 3–4 days weekly maximizes lean mass accretion and fat loss. High-intensity interval training (HIIT) complements strength work, improving cardiovascular capacity and metabolic health.
Sleep: Seven to nine hours nightly is foundational. Chronic sleep deprivation (five hours per night) cuts testosterone by 10–15% 9 — enough to undo treatment benefits. Sleep quality directly determines TRT efficacy.
Stress management: Chronic stress elevates cortisol, which suppresses testosterone and accelerates catabolism. Meditation, breathwork, social connection, and purposeful rest are as much a part of the protocol as the hormone itself.
Men who layer TRT with these lifestyle elements see compounded gains. Men who ignore lifestyle limitations plateau earlier.
Why Choose Zvia for Testosterone Therapy?
Testosterone replacement is straightforward at the pharmaceutical level: inject or implant, monitor labs, adjust if needed. But it’s a human-centered process at the clinical level — and that difference determines outcomes.
Zvia’s approach in Lakewood, Colorado rests on three pillars. First, comprehensiveness: Our initial lab panel includes over 70 markers — not just testosterone, but lipids, liver and kidney function, hemoglobin, PSA, metabolic markers, and inflammatory signaling. This baseline paints the full picture of your health, revealing opportunities to optimize alongside hormone therapy and flagging any risks before they emerge.
Second, precision monitoring: We track your testosterone levels regularly, especially in the first three to six months when fine-tuning is most valuable. We also monitor estradiol (to ensure the aromatase pathway is healthy, not suppressed or excessive), hemoglobin (to catch erythropoiesis changes early), lipid trends, and prostate health. Dosing adjusts based on labs and symptoms — not a formula, but a dialogue between your physiology and your protocol.
Third, integration with your life: We don’t prescribe testosterone in isolation. We ask about sleep, nutrition, training, stress, relationship satisfaction, and work demands. We understand that a hormone is most powerful when it meets a life that’s been tended — and that our job is to help you tend it.
This stands in sharp contrast to volume-focused telehealth models that mail a prescription based on a questionnaire, or to DIY approaches where men self-adjust without labs or clinical input. Zvia’s model asks: Who is this person? What do they need to thrive? How does testosterone fit into that picture? The answer is always personalized, always grounded in data, and always delivered with the care of a provider who knows you.
Educational purposes only. Provider-supervised protocols required. Results may vary based on individual biological response.
Discuss whether Testosterone is right for you with our clinical team.
References
- 1. Saad F, Aversa A, Isidori AM, et al. Onset of effects of testosterone treatment and time span until maximum effects are achieved . European Journal of Endocrinology (2011).
- 2. Lincoff AM, Bhasin S, Flevaris P, et al. Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE Trial) . New England Journal of Medicine (2023).
- 3. Handelsman DJ Androgen Physiology, Pharmacology, Use and Misuse . Endotext / NCBI Bookshelf (2024).
- 4. Kaminetsky JC, Bocchi L A Review of Testosterone Pellets in the Treatment of Hypogonadism . Current Sexual Health Reports / Springer (2015).
- 5. Barbonetti A, D'Andrea S, Francavilla S, et al. An updated systematic review and meta-analysis of the effects of testosterone replacement therapy on erectile function and prostate . Frontiers in Endocrinology (2024).
- 6. Luckett T, Grossmann M, Zajac JD, et al. The effects and safety of testosterone replacement therapy for men with hypogonadism: the TestES evidence synthesis and economic evaluation . Health Technology Assessment (2024).
- 7. Bhasin S, Brito JP, Cunningham GR, et al. Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline . Journal of Clinical Endocrinology & Metabolism (2018).
- 8. Walia T Testosterone Replacement, Where Are We in 2025? . Trends in Urology & Men's Health (2025).
- 9. Leproult R, Van Cauter E Effect of 1 Week of Sleep Restriction on Testosterone Levels in Young Healthy Men . JAMA (2011).
- 10. Shoskes JJ, Wilson MK, Spinner ML Pharmacology of testosterone replacement therapy preparations . Translational Andrology and Urology (2017).